“ Should Retinal Surgeons Influence the Selection of Intraocular Lens Implants?

©2004. Robert M. Kershner, M.D., M.S., F.A.C.S.
Eye Laser Consulting
Boston, Massachusetts USA. All rights reserved.
|
“ Should Retinal Surgeons Influence the Selection of Intraocular Lens Implants?
©2004. Robert M. Kershner, M.D., M.S., F.A.C.S. Eye Laser Consulting Boston, Massachusetts USA. All rights reserved. |
|
In ocular surgery’s early days, patients who had previously undergone cataract surgery sooner or later would fall into the domain of the retinal surgeon. Today, with better cataract surgery techniques, smaller incisions, and foldable intraocular lenses (IOLs), the occurrence of cystoid macular edema, vitreous loss, retinal tears and retinal detachment are much less common consequences of cataract removal 1 . When intraocular lenses replaced surgical aphakia in the late 70s, retinal complications concurrently decreased. Unfortunately, the widespread acceptance of IOL implantation did not come without it’s price. The presence of a small lens optic and an intact lens capsule all too often resulted in poorer visualization of the peripheral retina and a potential impediment to retinal treatment, especially in diabetics. The use of silicone material in a lens optic, further raised concerns as to the safety of using silicone oil in a retinal repair 2 .
Today’s IOLs, the product of an innovation developed in 1949 by the late Sir Harold Ridley, have undergone tremendous advances. There are 3-piece IOLs of foldable material, capsular “C” haptics to fixate the lenses within the capsular bag, and square-edged optics to reduce the incidence of posterior capsule opacification (PCO) 3 . With increasing advances in the technology of IOL design and manufacture, should retinal surgeons influence the type of IOL used in retinal patients? Certainly, there is a consensus amongst cataract surgeons that in diabetics, silicone IOLs should be avoided and an acrylic lens optic is selected. Is this the best choice? Is it based upon sound medical evidence or hearsay? The number one preferred optic material in use today is polyacrylamide or acrylic, as it is known. There are no studies supporting the long term safety of this material in the eye when compared with the over fifty year experience with polymethylmethacrylate (PMMA), and over thirty year experience with silicone. The choice of the lens optic material is made by the cataract surgeon based perhaps more on marketing and ease of implantation than evidence of medical study. Many feel that lens optic material affects the incidence of posterior capsular opacification (PCO) and a retinal surgeon’s view of the fundus. Recent clinical studies have demonstrated that it is lens design, optic edge configuration and haptic insertion that is most responsible for whether or not lens capsular epithelial cells migrate and opacify the capsule 3-5 .
The use of ultraviolet absorbing materials in IOL manufacture became readily accepted by the ophthalmic community in the 1980s. It’s acceptance is based upon the assumption that the human crystalline lens naturally absorbs wavelengths of light below 400nm. The risk of allowing penetrating wavelengths of light to pass through an artificial lens and damage the retina, spurred manufacturers to offer UV absorbing chromophores in all of their IOL optics. There was little downside to filtering UV light as it was easy to accomplish and posed no potential adverse effects. Studies show varying degrees of protection offered by today’s lenses 6 , nonetheless, utilizing UV absorbing IOLs is widespread and now an accepted fact.
IOLs also are being offered today that block the visible spectrum of light. Known as the “blue-blocker”, the yellow acrylic IOL absorbs light at 430nm which is a wavelength believed to be potentially damaging to the retinal pigment epithelium in culture 7 . There is however, no population based epidemiological studies to demonstrate that shielding the aging retina from the visible blue wavelength of light offers any protective advantage. Teleologically, it seems counterintuitive to filter out the predominant visible wavelength of light that floods the earth’s surface by day. Some have suggested that maximally blocking light at the precise wavelength that provides scotopic luminous efficiency for night tasks, such as driving, walking down a flight of stairs and viewing obstacles in a dark room, may make elderly patients less able to prevent falls and potential injury. Further study needs to be done in demonstrating a need for an IOL that has these potentially significant downsides.
When a retinal surgeon examines the fundus with an indirect ophthalmoscope, he or she uses an aspheric lens (usually a 20 diopter hand held condensing lens) to bring the light rays emerging from the scope’s illumination of the retina, to converge in focus in front of the eye. Why not use a simple spherical lens to accomplish the same purpose? The answer rests with the ability of an aspheric lens to neutralize spherical aberration induced by the cornea, to allow viewing of the peripheral retina without distortion. Can an IOL accomplish the same thing? In fact it can. Recent advances in IOL design involves applying wavefront technology to improve the optics and visual quality delivered through an IOL (Figure 1). This modified prolate anterior surface (MPAS) IOL, is known as the Tecnis™ (Advanced Medical Optics, Santa Ana, CA). The positive spherical aberration of the cornea, combined with a conventional spherical IOL results in reduced contrast sensitivity. In a study comparing the MPAS IOL with conventional spherical IOLs, the modified prolate optic successfully neutralized corneal spherical aberration, resulting in better contrast sensitivity, functional visual acuity 8 and patient safety.
Figure 1. The Tecnis™ IOL contains a modified prolate anterior surface which neutralizes spherical aberration.
A prospective randomized study compared the effects of the MPAS IOL with those of a conventional silicone lens (AA4207VF, Staar Surgical, Monrovia CA) and a conventional acrylic lens (AcrySof SA60AT, Alcon Surgical, Ft. Worth TX) on visual performance. The goal of the study was to determine whether the addition of the modified optic improves retinal imaging and functional visual performance. 221 eyes of 156 patients were randomized to receive one of the three IOLs. Test methods included Snellen visual acuity, digital retinal imaging, functional visual acuity, and contrast testing.
Results indicate that all three IOLs improved visual acuity after cataract surgery (with an average improvement of 20/35 or better). However, in the first month after surgery, patients implanted with the modified prolate lens had better uncorrected visual acuity compared to conventional spherical lenses.
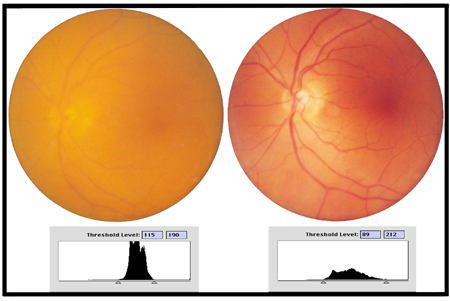
This study, in addition, measured retinal image contrast, by analyzing the threshold luminance of fundus images taken through the cataract preoperatively and through the IOL at one month postoperatively (Figure 2). The Tecnis IOL group demonstrated a 28% improvement in retinal imaging over conventional spherical IOLs.
Figure 2. Image of the fundus preoperatively on the left and postoperatively on the right demonstrating improved image contrast (corresponding histograms below each image).
So what does this tell us about IOL selection? Cataract surgeons must be cognizant of the potential for improvement in visual acuity and functional vision of their patients as a consequence of intraocular lens implantation. In following the primary doctrine, “physician, first do no harm” they must not select an IOL that has the potential to decrease visual potential or compromise the patient in any way from achieving the highest degree of visual functioning available with today’s technology. New standards are being created with new IOLs. The retinal surgeon should be aware of these changes and be prepared to argue strongly for that which is best for their patient’s vision and the surgeon’s ability to care for their needs should retinal intervention be required.
References:
1. Kershner, RM. "Clear Corneal Cataract Surgery and the Correction of Myopia, Hyperopia and Astigmatism." Ophthalmology 1997;104(3):381-389.
2. Seok, H, Chung, JW, et al. Phacoemulsification and foldable intraocular lens implantation combined with vitrectomy and silicone oil tamponade for severe proliferative diabetic retinopathy. Journal of Cataract and Refractive Surgery 30(8);1721-1726, 2004.
3. Kiran, A., Missier, A. et al. Posterior capsule opacification: silicone plate-haptic versus AcrySof intraocular lenses. Journal of Cataract and Refractive Surgery 29(8);1569-1574, 2003.
4. Hayashi, K, Hayashi, H, et al. Changes in posterior capsule opacification after poly(methyl methacrylate), silicone, and acrylic intraocular lens implantation. Journal of Cataract and Refractive Surgery 27(6);817-824, 2001.
5. Sacu, S, Meanpace, R. et al. Effect of intraocular lens optic edge design and material on fibrotic capsule opacification and capsulorhexis contraction. Journal of Cataract and Refractive Surgery 30(9);1875-1882, 2004.
6. Laube, T, Horst, A et al. Ultraviolet absorption of different intraocular lenses. Ophthalmology 111(5);880-885, 2004.
7. Sparrow, J, Miller, A, Zhou, J Blue light-absorbing intraocular lens and retinal pigment epithelium protection in vitro. Journal of Cataract and Refractive Surgery , 30(4);873-878, 2004.
8. Kershner, RM R etinal image contrast and functional visual performance with aspheric, silicone, and acrylic intraocular lenses Journal of Cataract and Refractive Surgery 29(9);1684-1694, 2003.
About the Author.
Dr. Kershner is a specialist in anterior segment surgery, a noted author and recognized lecturer internationally. He has no financial or proprietary interest in any of the materials described.
|