
HydroLasik with a New
LASIK Flap Forceps
Robert M. Kershner, MD, FACS
Eye Laser Center, Suite 303, 1925 West Orange Grove
Road, Tucson, AZ 85704-1152
Phone: (520) 797-2020, Fax: (520)-797-2235, e-mail: Kershner@asiteforeyes.com
©2002. Robert M.
Kershner, M.D., F.A.C.S.
LASIK has been well accepted as the surgical standard of care for the correction of refractive error. Unlike phacoemulsification for cataract surgery, which has relatively well-established application guidelines for its technology, the newness of LASIK has spawned a variety of techniques and instrumentation. For many LASIK surgeons, the confusion surrounding this bewildering array of techniques has led to a fear of potentially troublesome and devastating complications. The lack of universal acceptance of the techniques of LASIK has been hampered by the paucity of science to support one approach over another. Unfortunately, this has not escaped the attention of the media or the public and as a result, LASIK has lost some of it's luster. The reality however, is that LASIK works. It's accuracy, reproducibility, and rapid visual recovery still support it's acceptance as a present day state-of-the-art procedure for vision correction. Nonetheless, questions and controversy persist and problems with flap creation and handling continue to plague the LASIK surgeon.
Which excimer laser is best? What keratome should a surgeon use? Should a different keratome be selected for hyperopic treatments than for myopic? Which patients are good candidates, and which should be avoided? Should we use a thick flap or a thin flap? Should the flap have a nasal hinge or a superior hinge? Should the flap be kept dry or should it be wet? Should a flap be avoided altogether and LASEK employed as a modification of the older PRK technique? Should the LASIK patient be pretreated with antibiotics and antiinflammatory drops? Which drops should the postoperative LASIK patient use? These and many other questions continue to plague the refractive surgeon.
The answers to the above questions are not simple and are not without controversy. However, like phacoemulsification, surgeons can sort through the bewildering array of techniques and instruments and adopt a methodical, planned approach to lasik surgery that works consistently to assure a reproducible, precise, and successful procedure. I have embraced a simple method of flap construction and management that has been successful in my hands for several years. First developed for the automated lamellar keratoplasty procedure, I have now adopted my prior experience to the application of LASIK. In several thousand procedures over seven years, this method has shown itself to be simple to adopt and apply. It is associated with less complications such as flap damage, abrasions, epithelial ingrowth, striae and keratitis. When it comes to LASIK I have found that "wetter is better". The procedure I adhere to, I call HYDROLASIK.
The procedure is actually quite simple. I keep the steps few, the instruments minimal and the maneuvers simple. I utilize a single, clear, adhesive drape to cover the forehead and a clear tape to cover the lower eyelid. The eye is prepped with a wipe and topical 4% betadine drops are applied. Anesthesia is achieved with a few drops of topical proparacaine. The instruments are dry sterilized for each case. An aspiration speculum is inserted to keep secretions, tears and irrigation fluid off of the flap bed. The patient's treatment is reviewed by the surgeon and a last check of the data entry into the laser computer is verified. The keratome is selected and positioned over the cornea. For the majority of LASIK procedures I utilize a 180 to 200 micron thick flap for a 8.5mm overall flap diameter. For hyperopic ablations I prefer a 9.5mm overall diameter. The edge of the flap is marked with a dry, figure of eight marker, without ink. My studies have shown ink to be toxic to the epithelium and the stroma and occasionally can find its way into the interface, so I strongly advise against using it. Several drops of sterile balanced salt solution are placed onto the cornea beneath the keratome, prior to initiating the cut. The patient is instructed as what to expect and the position of the ring verified and the cut completed.
The key to successful flap construction is proper and consistent suction, smooth excursion of the keratome head with minimal surface friction. I prefer not to use keratomes which require on-eye assembly and instead prefer those with a one-handed operation such as the Becton Dickinson K-3000 keratome. I know that the controversy in flap thickness has not yet been solved, but my experience has shown that too thin flaps (less than 120 microns) are more often associated with flap problems. I therefore strive to create thick flaps. If I cannot achieve the full ablation depth and leave at least 300 microns of untouched corneal tissue in the bed (or 60% of corneal thickness), than I either will reduce the ablation or counsel the patient to consider an alternative treatment such as the implantable contact lens (ICL, STAAR Surgical, Monrovia, California). The flap is then created and pachymetry measurements of the flap and bed used to confirm the actual thickness.
The key to successful flap management is to avoid grasping or handling the flap or exposing the flap bed to potential contaminants. It is too tempting to use a forceps or hook to lift or grab the flap and to casually fold it over and position it for the laser application. It is flap handling however, that predisposes to abrasions, epithelial ingrowth, striae and keratitis. Surgeons need to avoid touching the undersurface of the flap with anything other than sterile balanced salt solution if complications are to be avoided.
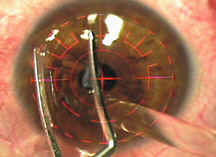
To aid in minimal handling of the flap, I have developed a specially designed flap forceps (Kershner LASIK Flap Forceps, Rhein Medical Tampa, Florida, product #8-16161) (Figure 1). Made of stainless steel with rounded handles for ease of handling and exquisite control, its direct action enables the surgeon to safely handle the flap without crimping or tearing it. The delicate, highly polished blades are designed to lift but not grab the flap edge. Its curved blades act like a very thin spatula to slide under the flap edge rather than pinch or grab it (Figure 2). The blades can lift the flap, flip the flap over in one-maneuver and reliably reposition the flap into its original configuration after laser application. The blades closely follow the contour of the cornea and when closed, the blades can be used to squeegee the flap to remove residual liquid in the interface, if required. The forceps are ideally configured to lift the flap without damaging the flap edge in instances of relifting the flap for retreatment.
The flap is gently lifted and positioned (Figure 3). The laser is aligned and the treatment applied. At this stage, many surgeons simply flip the flap back and quit. Alternatively, they may manipulate the flap while irrigating under it as they play with it's position. Both approaches are ill-advised. Repositioning the flap is of paramount importance to the success of LASIK. It is mandatory that surgeons reposition the flap exactly from where it came, that it's surface be smooth, that it is free of contaminants and foreign material, and that it is in the optimum state to attach to the now altered underlying stroma. To reposition the flap dry makes no sense. If the flap is dry, potential contaminants, debris and foreign bodies can adhere to the underside of the flap. As the flap falls to the bed, it can stick anywhere, not necessarily where it should rest and entrap unwanted particles. Because of this, I strongly believe that the bed as well as the underside of the flap be copiously irrigated with sterile, chilled balanced salt solution (Figure 4). Chilled irrigation cools the ablated tissue, minimizes swelling and allows the flap to float into the proper position. I simply use a liter bottle of irrigation fluid that has been kept in the refrigerator, hung on an IV pole, and connected to tubing with a sterile cannula on the end. When called for, the assistant opens the stopcock and the surgeon directs the stream of water onto the underside of the flap and into the flap bed. The aspirating speculum removes the excess fluid and dries the cornea as irrigation continues. I then use the one-step forceps to reposition the flap, align the edges and verify that the marks are in proper alignment (Figure 5). Any excess fluid can be squeegeed with the closed forceps (Figure 6). A dry cellulose sponge can be used to dry and verify that the edges of the flap and gutter are in correct alignment.
The strategy of using water at flap creation and to replace the flap, is based upon sound physical principles of corneal function. LASIK surgeons are well aware of the propensity of the flap to quickly adhere without the need for a patch or sutures. Why does this occur? Normally, the corneal endothelium is responsible for pumping water out of the corneal stroma into the anterior chamber to maintain the turgidity and clarity of the cornea. So strong is this vacuum pump from the epithelium towards the endothelium, that as much as 600mm Hg of pressure is created. This negative pressure creates an adherence and compression of the cornea stroma. When the superficial LASIK flap is created, there is a strong tendency for the flap to adhere due to this negative pressure gradient. That is why, even after cutting the flap free from the underlying stroma, the surgeon still must physically peel the flap off the cornea. The attraction is still strongly engaged. After application of the laser, the surface contour has been altered, but the vacuum pump from the endothelium is still functioning. Unfortunately, what it has been doing is to pump the stroma dry while the flap has been hydrating. This potentially creates a tissue mismatch.To assure the strongest attraction of the flap to the stromal bed requires water molecules to travel through the stroma. If the flap is repositioned dry, the pump has to work that much harder, and suction is easily broken. To facilitate the highest level of vacuum pressure, the endothelial pump must be primed with water to start the pumping of fluid through the stroma into the anterior chamber. The strategy of "wetting the bed" may not be wise when you were a child, but it sure works well for a corneal flap. Contrary to conventional thinking, irrigation actually makes the flap adhere better. It is the natural physiology of the cornea that makes this possible.
The patient should not instill eyedrops after the procedure. Hydrating the cornea after the flap has been properly positioned runs the risk of moving it, damaging it with drop instillation, or infiltrating undesirable molecules under the flap edge and into the interface. The postoperative lasik patient should rest with the eyelids closed for several hours. I do not use bandage contact lenses or occlude the operative eyes following the procedure. The patient needs to see and the eyelids need to blink to dehydrate the epithelium and assure a smooth flap and proper adhesion. The following day, after the epithelium has closed the flap edge, a topical antibiotic /antiinflammatory eyedrop can safely be started four times a day for one week. Artificial tear supplements are strongly encouraged, as all LASIK patients will experience symptoms of dry eye for at least several weeks following the procedure. To protect from the potential keratitis that can occur with sun exposure, ultraviolet protecting sunglasses are provided for all patients.
Using water as an adjunct tool in LASIK, is a technique I call HydroLASIK. With a jet of water, the flap can be carefully positioned without the need to grasp or hold it with a sharp instrument. This avoids the problems inherent in any forceps or cannula manipulation. Corneal abrasions, pinches and kinks in the flap can all be avoided if the only thing that touches the flap is water. In combination with the one-step flap forceps, HydroLASIK assures proper flap positioning and adherence. The likelihood of satisfactory flap repositioning is maximized and the potential for flap problems is avoided. This is easily accomplished without the need for multiple instruments or by adopting difficult maneuvers. In my experience, the potential risks of epithelial ingrowth, flap malpositions, striae, or keratitis are lessened with a wet technique. With today's LASIK procedure, water is truly our friend, "wetter is better"!
Robert M. Kershner, MD, FACS
is Director of Cataract and Refractive Surgery-Eye Laser Center Tucson, Arizona
USA, Clinical Professor of Ophthalmology, University of Utah School of Medicine,
Ik Ho Visiting Professor of Ophthalmology, Chinese University of Hong Kong and a
consultant specialist for Ophthalmic Surgical Product Development.
His offices are at the Eye Laser Center, Suite 303 1925 West Orange Grove
Road, Tucson, Arizona USA
85704-1152 Phone: (520)
797-2020 Fax: (520) 797-2235e-mail: Kershner@asiteforeyes.com
web site: http://www.asiteforeyes.com
Dr. Kershner has no
proprietary or financial interest in any of the devices or techniques described
in this article.
Legends to Figures:
(1) The Kershner Lasik Flap Forceps (Rhein Medical, Tampa, Florida)
(2) The Lasik Flap Forceps in position for use after flap creation with the microkeratome.

(3) The flat, polished, forcep blades are used to slip under the flap edge without disrupting it.

(4) After laser application, the bed and underside of the flap are irrigated with chilled balanced salt solution and the forceps is used to flip the edge of the flap.
(5) The forceps flips the flap into it's original position.

(6) The closed curved blades can be used to squeegee fluid from under the flap.
