©2005. Robert M. Kershner, MD, MS, FACS
Eye Laser Consulting
Boston, Massachusetts USA
In 1994, I published my results on the technique of clear corneal cataract surgery with the simultaneous correction of myopia, hyperopia and astigmatism. I called this approach “keratolenticuloplasty” (KLP) to reflect the surgical modification of the cornea along with correcting the lenticular error by replacing the natural lens with an IOL (1-2). The results of this technique demonstrated that we could improve uncorrected visual acuity with the cataract procedure. With the development of new lens designs, wavefront analysis, and even better surgical instruments and techniques, the science of vision correction and neutralization of refractive error has attained a new level with the cataract procedure (3-6).
I have been amazed, if not a bit disappointed, that ophthalmic surgeons did not immediately jump on the bandwagon to correct their patient’s refractive errors. The techniques were proven; the instruments finally available thanks to some enterprising and innovative new instrument and medical device manufacturers. Yet there we were, our patients still relegated to wearing spectacle correction for their astigmatism and presbyopia following cataract surgery. The increasing acceptance of refractive procedures to eliminate or reduce the need for spectacle and contact lens correction started gaining limited acceptance with the radial keratotomy technique of the late S. N. Fyodorov of Moscow, Russia. Even today, with the availability of laser technology, incisional keratotomy still provides the simplest, and most reproducible approach to astigmatic correction with cataract surgery. With today's state of the art cataract procedure patients now demand and should expect unaided clear vision. The push for emmetropia with phakic, aphakic bifocal and accommodative IOLs has finally created an impetus for all surgeons to deliver an eye free from refractive error, especially astigmatism. The patient's visual results and immediate recovery without restriction speak for themselves . Eighty-nine percent of all patients are spectacle-free for most tasks. What good is implanting an accommodative IOL (Crystalens™, Eyeonics, Aliso Viejo, CA) if the patient has to wear glasses for astigmatism? Here is how you can combine these techniques with your procedures.
Preoperative Evaluation and Surgical Plan:
The strategy for your IOL patients is to correct the sphere fully for distance, eliminate more than 0.75 (D) of astigmatism with a single incision keratotomy that can also double as the IOL insertion site. Aim for full correction or slightly undercorrect the cylinder, NEVER overcorrect or shift the cylinder axis. To avoid the possibility of error, I utilize a preoperative surgical plan.
Limbal relaxing Incisions (LRIs) are a misnomer. The incisions made into the cornea to flatten are neither relaxing nor limbal. Where you make the incision is just as important as how you make it. Prior to surgery note in the chart the position of the patient’s steepest meridian on the cornea (consult a worksheet). Carefully evaluate the patient’s preoperative astigmatism and take a topographic map with you into the operating room. Corneal incisions can consistently and predictably alter the corneal curvature. First described by Spencer Thornton, MD of Nashville, Tennesse, one of the early American pioneers in refractive keratotomy, all transverse or arcuate corneal incisions will flatten the cornea in the meridian in which they are placed by acting as if tissue had been added to the keratotomy site.
How best can a surgeon flatten the cornea with an incision?
I have long been a champion of a single, small arcuate incision (AK) on near clear cornea at an optical zone of about 10mm. If a single incision won’t do the job, simply pair it with another on the opposite meridian. How do arcuate astigmatic incisions differ from limbal relaxing incisions? Limbal relaxing incisions, because they are placed far peripherally in the cornea at the scleral limbus and furthest from the optical center of the eye, have less flattening effect for a given length. As a result, they must be large to have any substantial effect on corneal curvature. When limbal incisions exceed 120 degrees of arc, especially if they are placed nasally or temporally, they effectively denervate the cornea at that location, creating dry eye and healing problems. Smaller, arcuate incisions (usually 3.0 mm), which closely follow the natural curvature of the cornea have more effect with less cutting and little downside risk. Follow a published nomogram, use the right tools, and make the incision deep enough (at least 85-95% corneal thickness to have a permanent effect (see below) and the results are highly predictable.
Instruments for Astigmatic Keratotomy
I have been very pleased to see the large number of astigmatic keratotomy instruments now available from a large number of manufacturers. I will just mention three as examples. To make the AK, use topical anesthesia, so the patient can fixate on the OR microscope light, and for safety sake, use a Thornton style ring to fixate the globe. Mark the location of the AK on the steepest meridian using the Kershner astigmatic markers available from Rhein (Rhein Medical, Tampa, FL). If you prefer the sharpness of the diamond blade and have the pocket book and staff to purchase and maintain one, I prefer the Kershner astigmatic keratotomy blade from Diamatrix (Diamatrix, The Woodlands, TX), Mastel (Mastel Precision, Fargo ND), or the Seibel LRI Diamond Knife from Rhein. You can’t beat a diamond for a smooth, reproducible, full depth incision. For diamond like quality in a disposable product, I recommend the BD Atomic Edge™ Blade (BD Ophthalmic Systems, Waltham, MA) made from silicon semiconductor material.
A new addition to creating the astigmatic keratotomy, is a device that is about as idiot proof as it gets, the Terry/Schanzlin Astigmatome (Oasis Medical, Glendora, CA). This extremely clever device incorporates a vacuum speculum, a series of single and double disposable blade units and various template sets to allow the construction of any length and optical zone incision automatically. Get your hands on a set of nomograms, a good video or DVD of the technique, and practice. A little diligence pays off in emmetropic and very happy patients.
Dr. Kershner is President and CEO of Eye Laser Consulting in Boston, Massachusetts. He has no proprietary or financial interest in any device or technique mentioned in this article.
Figures
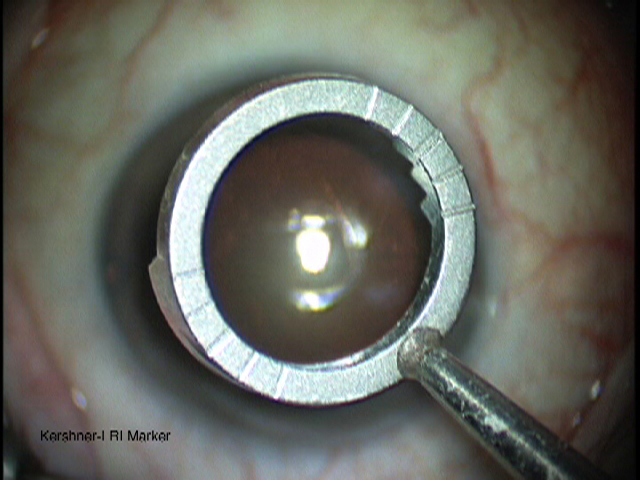
• Fixate the globe and mark the location of the AK.

• An arucate keratotomy incision is made 85-95% depth perpendicular to the cornea at near clear limbus.
For published nomograms go to:
References:
- Kershner RM. Refractive Keratotomy for Cataract Surgery and the Correction of Astigmatism . Thorofare, NJ: Slack, Inc., 1994, 141 pages.
- Kershner RM. “Keratolenticuloplasty.” Surgical Treatment of Astigmatism . Eds. Gills JP, Sanders DR. Thorofare, NJ: Slack, Inc., 1994, pp. 143-155.
- Kershner RM. “Keratolenticuloplasty - Arcuate Keratotomy for Cataract Surgery and Astigmatism.” Journal of Cataract and Refractive Surgery 1995;21(3):274-277.
- Kershner, RM. “Clear Corneal Cataract Surgery and the Correction of Myopia, Hyperopia and Astigmatism.” Ophthalmology 1997;104(3):381-389.
- Kershner, RM “Optimizing the Refractive Outcome of Clear Cornea Cataract Surgery” Highlights of Ophthalmology- Phaco, Phakonit and Laser Phaco-A Quest for the Best, Benjamin Boyd, MD, Eds. Agarwal, S, Agarwal, A, Agarwal, A., Slack, Inc., Chapter 9, 2002.
- Kershner, RM "Refractive Keratotomy and the Toric IOL for the Correction of Astigmatism in Clear Cornea Cataract Surgery " in James Gills, M.D., Editor A Complete Guide to Astigmatism Management, Slack, Inc. 2002.